
A torn meniscus is among the most frequent knee injuries. It can occur during activities that involve forceful twisting or rotation of the knee, particularly when bearing your full body weight.
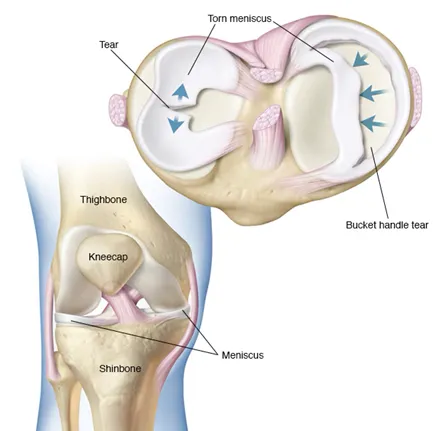
The knee contains two menisci, a medial and lateral meniscus, which individually are C-shaped cartilage structures that serve as cushions or shock-absorber between the shinbone and thighbone.
A torn meniscus can result in pain, swelling, stiffness, difficulty fully extending the knee, feeling of your knee giving way and a sensation of the knee being “blocked” during movement.
What is a partial meniscectomy for meniscus tear?
A partial meniscectomy involves removing a damaged portion of the meniscus, a C-shaped cartilage in the knee that acts as a shock absorber, protecting the joint. This procedure is performed when the tear’s configuration or severity makes repair impossible. The goal is to alleviate pain and restore knee function while preserving as much of the meniscus as possible.

When is partial meniscectomy necessary?
- Tears that cannot be repaired due to location or pattern.
- Severe pain and restricted knee movement caused by the tear.
- Cases where preserving the meniscus would compromise knee stability.
What are the benefits of meniscal surgery?
If knee symptoms persist despite rehabilitation efforts, meniscal surgery can help alleviate discomfort, improve mobility, and make further rehabilitation more effective.
Is meniscal surgery right for me?
Meniscal surgery is typically recommended when symptoms cannot be managed through non-surgical methods.
A consultation with your surgeon will help determine if surgery is the most suitable option for your condition.
What happens during partial meniscectomy surgery?
Meniscal surgery is commonly performed arthroscopically (keyhole surgery) under general anaesthesia.
Your surgeon will make small incisions in your knee to access the meniscus using specialised surgical instruments and a miniature camera.
The damaged meniscus section is carefully trimmed and removed.
Preservation of healthy meniscus tissue is important to maintain knee function.

What is the recovery time frames following knee partial meniscectomy surgery?
The knee arthroscopy procedure involving partial meniscectomy, causes minimal tissue damage.
Most patients recover relatively quickly.
- Hospital stay: Patients typically are discharged the same day following surgery.
- Pain management: Medications and physiotherapy help manage postoperative pain.
- Rehabilitation: Exercises to strengthen muscles and improve joint movement start shortly after surgery. Before discharge, a physiotherapist will guide you on gentle exercises and how to use stairs safely. They will provide initial advice tailored to your specific surgery.
Time frames and post-op rehabilitation will depend on the exact treatment carried out during the surgery and should always be confirmed by your surgeon for individual cases.
As a general guide:
- 1–2 days after surgery
- You can eat and drink shortly after the procedure and should be able to walk, though crutches may be necessary for support.
- Avoid long walks or prolonged standing. When climbing stairs, lead with your good knee going up and your treated knee coming down.
- 3 days after surgery
- The surgeon will often recommend removing the wool and crepe bandage at 72 hours following the surgery, but to leave the ‘sticky wound dressings on’. This needs to remain in situ till wound inspection by a health care professional usually at 2 weeks. It is critically important to keep the wound dry during healing which can take up to 3 weeks and so protect it when having a shower. Before leaving the hospital, your healthcare team will provide detailed instructions on wound care.
- 1–2 Weeks after surgery
- Some patients may still observe pain and swelling and should still avoid overexerting themselves.
- Elevation of the knee using a pillow under the foot at nighttime, and application of ice can help reduce swelling more quickly.
- Physiotherapy exercises are important.
- 2 Weeks after surgery
- A wound check is advised by a healthcare professional to ensure all has healed as expected and stitches removed.
- 6–12 Weeks After Surgery
- Most patients feel significantly recovered by six weeks, though some may need up to 12 weeks to feel fully normal.
- Recovery time varies depending on your condition and the procedures performed.
- Follow-up appointments with your surgeon at approximately 6-8 weeks are important. During this visit, the surgeon will assess for wound healing, knee movement, and determine the need for additional physiotherapy.
- Returning to Sports
- Avoid sports until the swelling subsides and your knee is strong enough to handle exercise.
- Your orthopaedic surgeon and physiotherapist will guide you on the appropriate timeline to resume sports safely.
- Returning to work
- Before going back to work, consult your surgeon for personalised advice as it will depend on the treatment carried out within the knee. As a general guideline:
- For desk jobs, you can typically return to work approximately two weeks after surgery.
- Physically demanding roles may require up to four weeks of recovery before returning.
- Returning to driving
- Refrain from driving until knee pain, swelling, and stiffness are resolved, and you regain full movement.
- You may be able to drive again approximately six weeks after your surgery, although this timeframe can vary between individuals. Your consultant will provide specific guidance based on your progress.
- Do not drive until you feel confident in controlling your vehicle and always confirm with both your surgeon and your insurance provider before resuming driving.
What is the follow-up following surgery?
- A wound check and removal of stitches (if used) will be required at approximately 14 days after your surgery with a healthcare professional.
- A routine follow-up appointment with your surgeon will be needed around 6–8 weeks after your surgery.
How soon can you fly after knee partial menisectomy surgery?
There is no specific formal medical guidance with respect to how long after surgery it might be before you are safe to fly.
Most surgeons and airlines recommend you should not fly within 6 weeks of surgery because of the increased risk of developing blood clots (Deep vein thrombosis, pulmonary embolism).
Please check with your surgeon for any advice regarding air travel and any precautions to take if you have additional risk factors for blood clots.
What is the recovery and rehabilitation?
- Typically faster recovery than repair procedures.
- Most patients regain mobility within weeks.
- No knee brace required; weight-bearing is often allowed sooner.
- Rehabilitation focuses on strengthening and restoring function.
Considerations and Outcomes
While a partial meniscectomy is effective in pain relief, the loss of even a portion of the meniscus can affect knee biomechanics. Long-term implications may include an increased risk of osteoarthritis, especially if significant cartilage damage is present.